1601006110 LONG CASE
1601006110
This is an online E log book to discuss our patient\"s de-identified health data shared after taking his/her/guardian\"s signed informed consent. Here we discuss our individual patient\"s problems through series of inputs from available global online community of experts with an aim to solve those patient\"s clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment
HALL TICKET :1601006110
A 45 year old male resident of Nalgonda labourer by occupation presented with chief complaint of :
• Shortness Of Breath since 10 days
• Cough since 10 days
• Pedal Edema since 10 days
History of presenting Illness:-
Patient was apparently asymptomatic 10 days ago,then developed —
• Grade III shortness of breath which was insidious in onset , nonprogressive,aggravated by walking and strenous work and dressing , relieved by sitting
There is history of orthopnea
There is no history of PND
• Dry Cough since 10days which is insidious in onset , non progressive ,no aggrevating and relieving factors
• Grade III bilateral Pedal edema since 10 days which in insidious in onset , gradually progressive,pitting type , no aggravating and no relieving factors
.
Fever since 10 days which is insidious in onset ,with evening rise of temperature , intermittent , not associated with chills and rigors , headache , vomiting
• History of burning micturition and oliguria since 5 days
• There is no history of sweating , palpitations , chestpain , hematuria
Past history
• 2 years back he developed symptoms of productive cough and fever for 1 week for which he visited to hospital and diagnosed with TUBERCULOSIS and took antitubercular drugs for 6 months and at that time he was told be having some kidney issues and used some medications ( records notavailable )
• Not a known case of diabetes ,hypertension,asthma , convulsions
• Surgical history is not significant.
Family history
Not significant
Personal history
• Decreased appetite
• Mixed diet
• Regular bowel habits and normal
• Patient has oliguria and burning micturition
• He is an alcoholic since 10 years , drinks once weekly
• Smoker since 25 years , he smokes daily 2-5 beedis
GENERAL EXAMINATION
Patient is conscious coherent and cooperative , moderately built , moderately nourished
⁃ Presence of pallor
⁃ No icterus , no cyanosis, no clubbing ,no pedal edema
⁃ No generalized lymphadenopathy

Vitals
⁃ Pulse taken in sitting position ,left radial pulse ,Pulse rate : 80bpm , regularly regular
⁃ BP 130/80 mmHg measured in sitting position on right upper arm
⁃ Respiratory rate : 20cpm
⁃ Afebrile
RESPIRATORY SYSTEM EXAMINATION
Patient is examined in supine aswell as in sitting positions under well ventilated room with consent taken
Upper respiratory tract :
nose , oral cavity are examined and no abnormal findings are present
examination of chest proper :
- Inspection
⁃ shape of chest : normal
⁃ Symmetry of chest : symmetrical
⁃ Trial sign negative
⁃ Movements of chest : RR -20cpm .
Type - abdomino thoracic.
. Equal on both sides
⁃ No involvement of accessory muscles and no intercoastal tenderness
⁃ No visible scars , no sinuses , no engorged veins
⁃ No deformities of spine
⁃ No visible apical impulse

- palpation
⁃ No tenderness and no local rise of temperature
⁃ Inspectory findings are confirmed
⁃ Trachea central
⁃ Apex beat : felt at 5 th Intercoastal space medial to mid clavicular line
⁃ Decreased chest expansion
⁃ Vocal fremitus : decreased at infra axillary and infra scapular areas on both sides normal on supra clavicular , infraclavicular ,mammary , infra mammary , suprascapular and interscapular areas
.
- Percussion
- Direct percussion: resonant on clavicle , sternum
2. Indirect percussion :
Anterior :
⁃ resonant in supra clavicular area
⁃ Resonant in infraclavicular area
⁃ Resonant in inframammary area on both sides
⁃ Traube’s space:dull
Posterior :
⁃ Resonant in suprascapular area
⁃ Resonant in interscapular area
⁃ Dull in Infrascapular area on both sides
- Auscultation
⁃ Bilateral air entry present
⁃ Normal vesicular breath sounds heard
Reduced in B/ L infrascapular and infra axillary areas
- fine crepts heard on B/L infra axillary and infra scapular areas
CVS EXAMINATION
⁃ S1 S2 heard
⁃ No murmurs
⁃ No palpable thrills
ABDOMINAL EXAMINATION
Scaphoid shape
No tenderness
No palpable mass
No hepatosplenomagaly
No ascites
Bowel sounds present
CNS EXAMINATION
⁃ Conscious and alert
⁃ Normal gait
⁃ Normal speech
⁃ No signs of meningeal irritation
⁃ Cranial nerves , motor system , sensory
⁃ Reflexes : superficial and deep tendon reflexes are intact
INVESTIGATIONS
⁃ CBP
⁃ CUE
⁃ Abg
⁃ RFT
⁃ LFT
⁃ PT
⁃ APTT
⁃ Blood sugar
⁃ ESR
⁃ Serum pottasium
⁃ Blood culture
⁃ Chest x ray
⁃ Ecg
⁃ Ultrasound abdomen




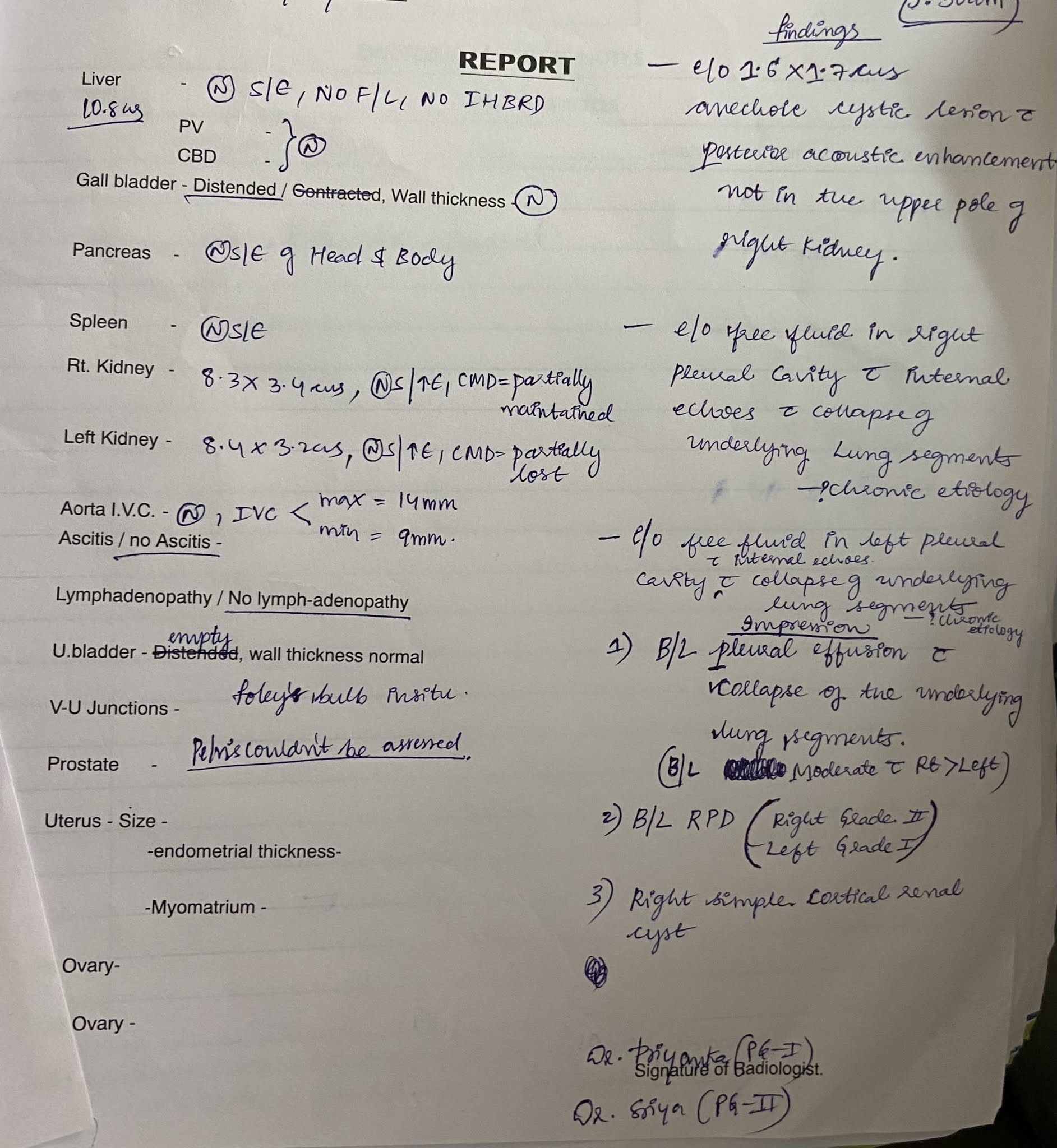

Provisional diagnosis :ACUTE ON CHRONIC RENAL FAILURE with pleural effusion and past history of PULMONARY TUBERCULOSIS .
TREATMENT
⁃ Salt and fluid restriction
Salt - < 2 g/ day
Fluid - < 1 lt / day
⁃ Injection iv LASIX 40mg BD
⁃ Tab NODOSIS 500mg bd
⁃ Tab SHELCAL 500mg od
⁃ Input and output charting
⁃ Bp pulse spo2 charting

















Comments
Post a Comment