1601006172 LONG CASE
50 year old with Weakness of left half of the body
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and diagnosis with a treatment plan.
This is an online E log book to discuss our patient’s de-identified health data shared after taking her guardian’s signed informed consent.
Hall ticket number: 1601006172
Date of admission: 20/4/2021
Date of examination of patient: 24/4/2021
A 50 year old right handed lady, who is a farmer by occupation, hailing from Vardhamanapeta came with
Chief Complaints:
- Weakness of left upper limb and lower limb since 5 days.
- Slurring of speech since 5 days.
- Deviation of angle of mouth to right since 5 days.
History of Presenting illness:
She was apparently asymptomatic 5 days back.
On 20th of April,
She woke up and did her routine activities like brushing and cooking food.
At 8:30 AM, she went to wash her face and experienced weakness of Left Upper limb and Lower limb, which was sudden in onset, leading to a fall associated with loss of consciousness from which she recovered spontaneously 5 minutes later.
She complains of giddiness at the beginning of attack.
She also experiences slurring of speech which was sudden in onset and gradually progressive.
This is associated with drooling of saliva and deviation of angle of mouth towards right side while speaking, eating and showing teeth.
She is unable to comb her raise and mix her food.
She is unable to squat and has difficulty in wearing slippers.
She was brought to the hospital at 6pm.
There is no history of involuntary movements.
No history of loss of bowel and bladder control.
No history of vomiting, convulsions, double vision, nasal regurgitation or nasal intonation.
No history of head injury, fever, palpitations, chest pain or breathlessness.
No history of similar attacks in the past.
No history of memory impairment.
No history of waxing or waning of symptoms.
Past History:
No history of similar complaints in past.
She is a known case of Hypertension and Type 2 diabetes mellitus since 8 years and is on medication for it.
There is no history of tuberculosis, bronchial asthma, COPD, rheumatic fever or epilepsy.
No history of recent weight loss.
Past Surgical History
She underwent hysterectomy for fibroids 9 years ago.
Drug history:
She has been taking the following drugs since 8 years:
- Telmisartan 40 mg
- Teneligliptin 20mg
- Glimepiride 0.2mg,Voglibose 0.2mg and Metformin 500mg
No history of any drug allergies.


Family history:
No history of similar attacks in other family members.
Personal history:
Diet: mixed
Appetite: normal
Sleep: adequate
Bowel and bladder movements: regular
No addictions
General examination:
The patient is conscious, coherent and cooperative.
She is moderately built and moderately nourished.
She is lying in supine position in the bed.
Temperature: afebrile
Pulse: 78/minute, regular, normal in volume, no thickening of arterial wall felt, No radio radial or radio femoral delay seen.
Blood Pressure: 130/90 mm Hg recorded on right arm in supine position.
Respiratory rate: 18 cycles/minute
Pallor: absent
Icterus: absent
Cyanosis: absent
Clubbing: absent
Koilonychia: absent
Lymphadenopathy: absent
Edema: present and of pitting type

Systemic examination
Central Nervous System examination
The patient is conscious, alert and cooperative.
A) Higher mental function
She is oriented to time, place and person.
Her speech is slurred.
Her comprehension is intact and repetition is normal.
B) Cranial Nerves
- Olfactory (I): can perceive smell
- Optic (II): Visual acuity- CF 2 in both eyes and field of vision- normal
- Occulomotor(III), Trochlear(IV),Abducens(VI) : External ocular movements full in all directions. No nystagmus and no ptosis. Pupil reactive to light.
- Trigeminal Nerve: Sensation over face present. Corneal reflex and Jaw jerk present.
- Facial Nerve (VII): deviation of angle of mouth to right side. Loss of nasolabial fold on left side. Frowning present, upper half of face escaped. Drooling of food particles on left side.
-
- Vestibulocochlear nerve(VIII): audition intact on both sides.
- Glossopharyngeal(IX) and Vagus(X): gag reflex present.
- Accessory(XI) and hypoglossal nerve(XII): normal

C) Motor function
Nutrition: no wasting seen.
Tone R. L
Upper limb. Normal. Decreased
Lower limb. Normal. Decreased
Muscle power
Upper limb. 5/5. 1/5
Lower limb 5/5. 3/5
No involuntary movement.
D)Sensory function
Superficial: pain, touch and temperature are intact.
Deep: vibration sense, muscle sense, pressure sense, joint sense and position sense are intact.
Cortical: one point localization, two point discrimination, stereognosis and graphaesthesia intact
E) Reflexes
Superficial
Right. Left
Abdominal Normal. Lost
Plantar reflex Flexor. Extensor
Deep
Biceps jerk. +2. +2
Triceps jerk. +2. +1
Supinator jerk. +1. -
Knee jerk. +2. +2
Ankle jerk. - -
Clonus Absent. Absent
Visceral
Swallowing: normal
Bladder: normal
Bowel: normal
F) Trophic Changes: absent
G) Cerebellar function
Dysdiadochokinesia: absent.
No nystagmus
H)Autonomic function: normal
Cardiovascular system
Peripheral arterial pulses: present
Carotid pulsations present, no Bruit heard.
S1 and S2 heard. No murmurs.
Respiratory System
Shape of chest: Elliptical
Movement of chest: normal
Trachea: central in position
Percussion: resonant on both sides
Breath sounds: vesicular
Vocal resonance: normal on both sides
Adventitious sounds: none
Gastrointestinal Tract
Mouth, tongue, teeth, gum: Normal
Bowel sounds heard
Investigations
1. Chest X ray

2. CT Head

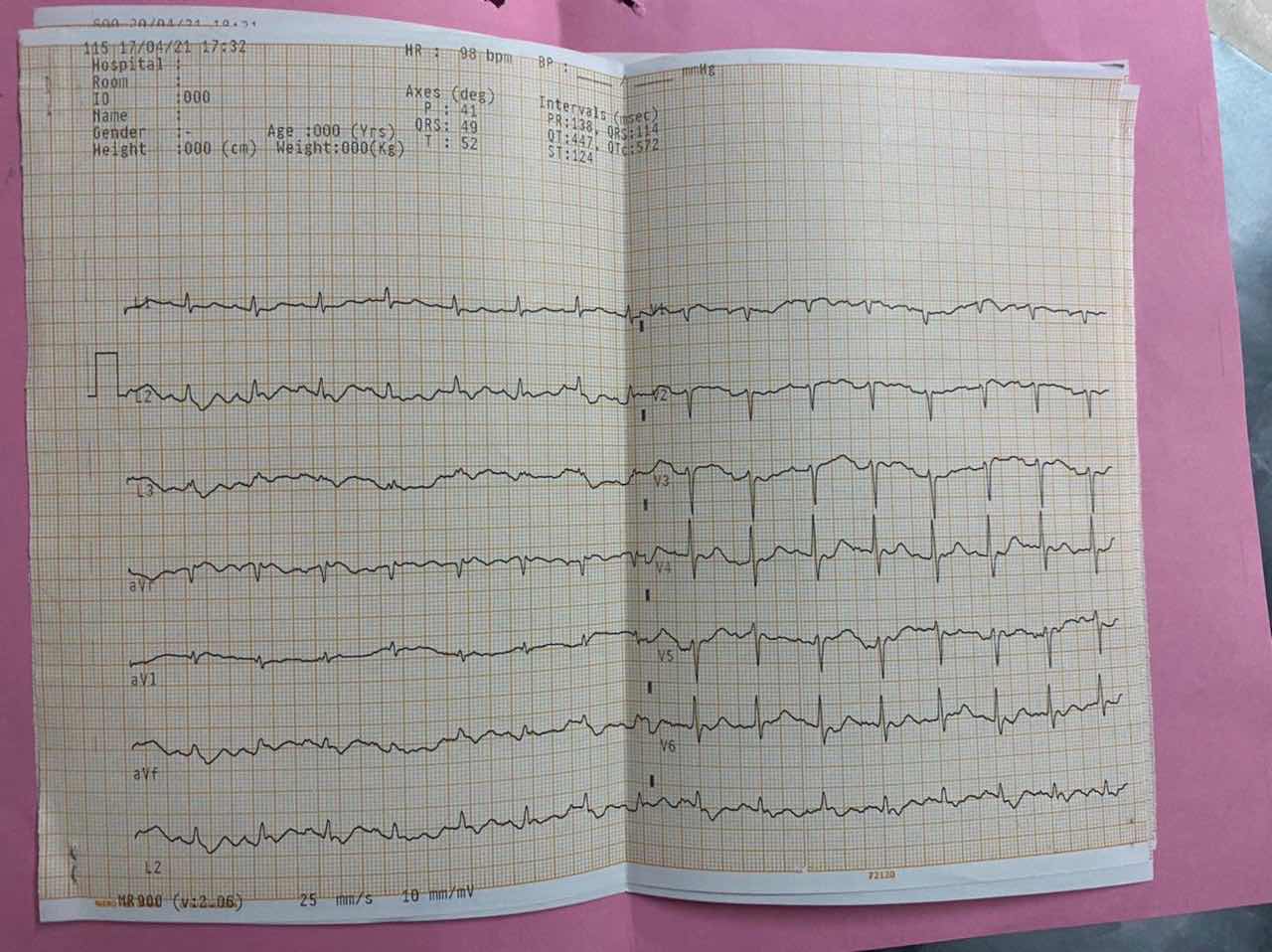
3. ElectroCardioGram
Treatment
1. Pharmacotherapy:
- Rosuvastatin ( HMG CoA inhibitor) given to decrease the risk of stroke in the future.
- Pregabalin and Methylcobalamine: to treat nerve damage

2. Physiotherapy
Provisional diagnosis:
Left sided hemiplegia with Left VIIth nerve palsy
Based on the history,
- Anatomical localization: Infarct of Middle cerebral artery supplying the Right Internal Capsule. It is an upper motor neuron lesion. Upper motor neuron lesion of the VII nerve leading to facial nerve palsy on the same side of hemiplegia suggests that the lesion is above the pons.
- Pathological abnormality: Ischemia
- Biochemical abnormality: free radical release due to hypoxia
- Physiological abnormality: weakness of left upper limbs, lower limbs and left side of face.

Comments
Post a Comment