1601006047 LONG CASE
HALL TICKET :1601006047
A 45 year old male resident of Nalgonda labourer by occupation presented with chief complaint of :
• shortness of breath since 10 days
• Cough since 10 days
• Pedal edema since 10 days
History of presenting illness
Patient was apparently asymptomatic 10 days ago,then developed —
• Grade III shortness of breath which was insidious in onset , nonprogressive,aggravated by walking and strenous work and dressing , relieved by sitting
There is history of orthopnea
There is no history of PND
• Dry Cough since 10days which is insidious in onset , non progressive ,no aggrevating and relieving factors
• Grade III bilateral Pedal edema since 10 days which in insidious in onset , gradually progressive,pitting type , no aggravating and no relieving factors
. fever since 10 days which is insidious in onset ,with evening rise of temperature , intermittent , not associated with chills and rigors , headache , vomiting
• History of burning micturition and oliguria since 5 days
• There is no history of sweating , palpitations , chestpain , hematuria
Past history
• 2 years back he developed symptoms of productive cough and fever for 1 week for which he visited to hospital and diagnosed with TUBERCULOSIS and took antitubercular drugs for 6 months and at that time he was told be having some kidney issues and used some medications ( records notavailable )
• Not a known case of diabetes ,hypertension,asthma , convulsions
• Surgical history is not significant.
Family history
Not significant
Personal history
• decreased appetite
• Mixed diet
• Regular bowel habits and normal
• Patient has oliguria and burning micturition
• He is an alcoholic since 10 years , drinks once weekly
• Smoker since 25 years , he smokes daily 2-5 beedis
GENERAL EXAMINATION
Patient is conscious coherent and cooperative , moderately built , moderately nourished
⁃ Presence of pallor
⁃ No icterus , no cyanosis, no clubbing ,no pedal edema
⁃ No generalized lymphadenopathy


Vitals
⁃ Pulse taken in sitting position ,left radial pulse ,Pulse rate : 80bpm , regularly regular
⁃ Bp 130/80 mm hg measured in sitting position on right upper arm
⁃ Respiratory rate : 20cpm
⁃ Afebrile
RESPIRATORY SYSTEM EXAMINATION
Patient is examined in supine aswell as in sitting positions under well ventilated room with consent taken
Upper respiratory tract :
nose , oral cavity are examined and no abnormal findings are present
examination of chest proper :
- Inspection
⁃ shape of chest : normal
⁃ Symmetry of chest : symmetrical
⁃ Trial sign negative
⁃ Movements of chest : RR -20cpm . .
Type - abdomino thoracic.
. Equal on both sides
⁃ No involvement of accessory muscles and no intercoastal tenderness
⁃ No visible scars , no sinuses , no engorged veins
⁃ No deformities of spine
⁃ No visible apical impulse

- palpation
⁃ No tenderness and no local rise of temperature
⁃ Inspectory findings are confirmed
⁃ Trachea central
⁃ Apex beat : felt at 5 th Intercoastal space medial to mid clavicular line
⁃ Decreased chest expansion
⁃ Vocal fremitus : decreased at infra axillary and infra scapular areas on both sides normal on supra clavicular , infraclavicular ,mammary , infra mammary , suprascapular and interscapular areas
.
- Percussion
- Direct percussion: resonant on clavicle , sternum
2. Indirect percussion :
Anterior :
⁃ resonant in supra clavicular area
⁃ Resonant in infraclavicular area
⁃ Resonant in inframammary area on both sides
⁃ Traube’s space:dull
Posterior :
⁃ Resonant in suprascapular area
⁃ Resonant in interscapular area
⁃ Dull in Infrascapular area on both sides
- Auscultation
⁃ Bilateral air entry present
⁃ Normal vesicular breath sounds heard
Reduced in B/ L infrascapular and infra axillary areas
- fine crepts heard on B/L infra axillary and infra scapular areas
CVS EXAMINATION
⁃ S1 s2 heard
⁃ No murmurs
⁃ No palpable thrills
ABDOMINAL EXAMINATION
Scaphoid shape
No tenderness
No palpable mass
No hepatosplenomagaly
No ascites
Bowel sounds present
CNS EXAMINATION
⁃ Conscious and alert
⁃ Normal gait
⁃ Normal speech
⁃ No signs of meningeal irritation
⁃ Cranial nerves , motor system , sensory
⁃ Reflexes : superficial and deep tendon reflexes are intact
INVESTIGATIONS
⁃ CBP
⁃ CUE
⁃ Abg
⁃ RFT
⁃ LFT
⁃ PT
⁃ APTT
⁃ Blood sugar
⁃ ESR
⁃ Serum pottasium
⁃ Blood culture
⁃ Chest x ray
⁃ Ecg
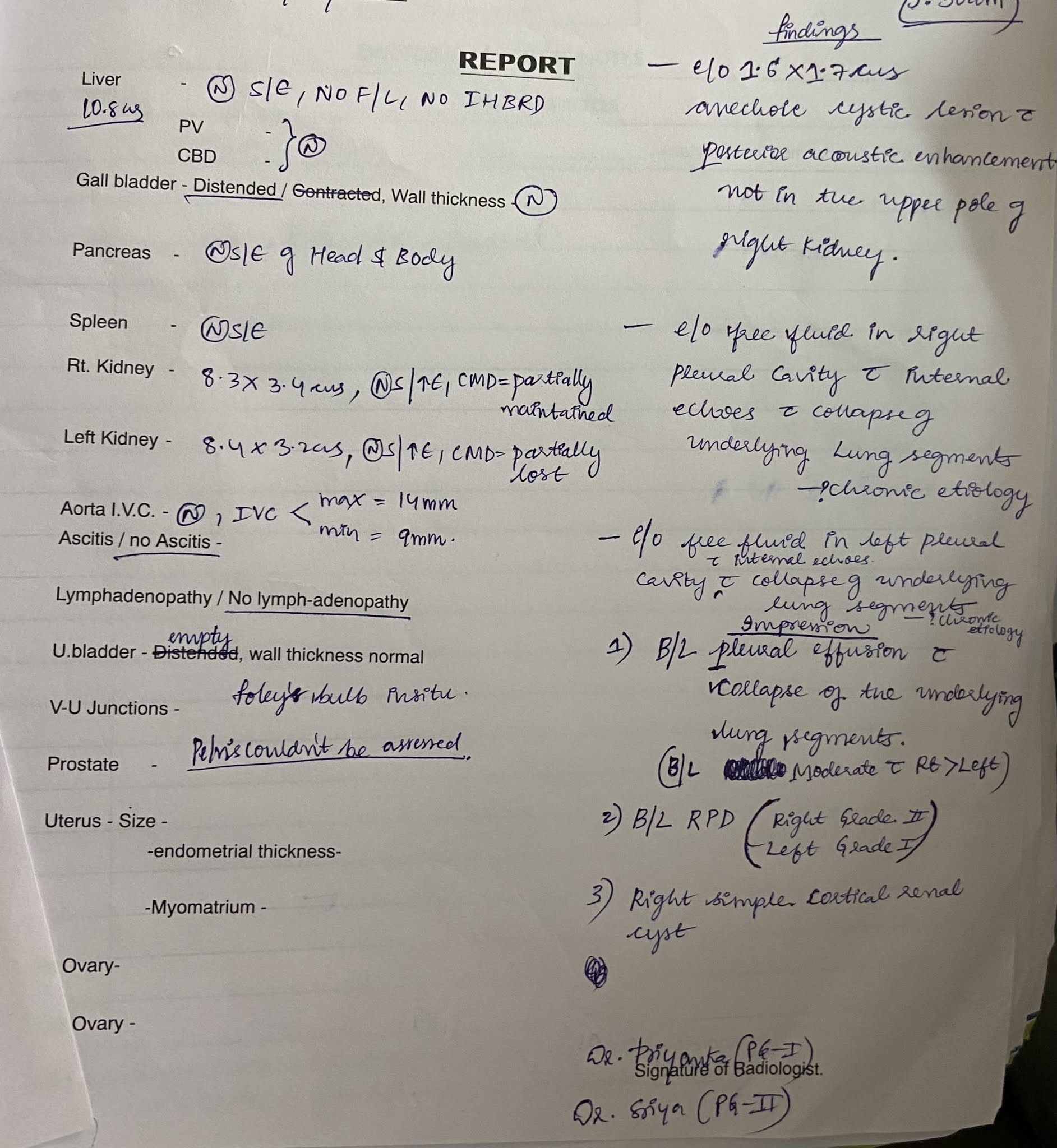
⁃ Ultrasound abdomen





Provisional diagnosis :ACUTE ON CHRONIC RENAL FAILURE with past history of pulmonary TUBERCULOSIS
TREATMENT
⁃ Salt and fluid restriction
Salt - < 2 g/ day
Fluid - < 1 lt / day
⁃ Injection iv LASIX 40mg BD
⁃ Tab NODOSIS 500mg bd
⁃ Tab SHELCAL 500mg od
⁃ Input and output charting
⁃ Nebulization with mucomist and BUDICORT 12 th hrly
⁃ Bp pulse spo2 charting













Comments
Post a Comment